
Hala Kfoury
Hala Kfoury Kassouf is Associate Professor of Pathology at the King Saud University Hospital in Saudi Arabia.
Case #17: S13-2744. Acute post-infectious glomerulonephritis.
Case #16: H11-2873. C3 Glomerulonephritis.
Case #15: H13-6814: Acute tubulo-interstitial nephritis (Sjogren Syndrome)

Case #14: H11-4326 Renal Dysplasia.
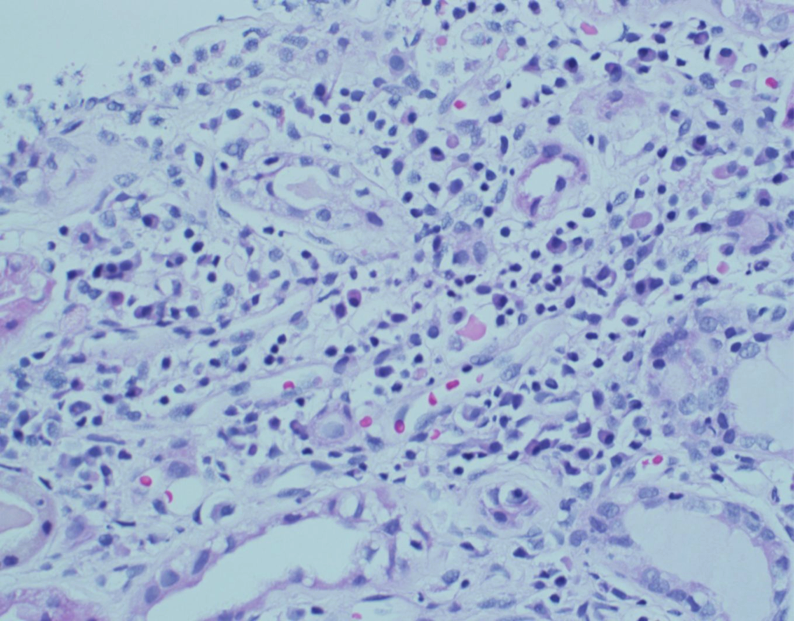
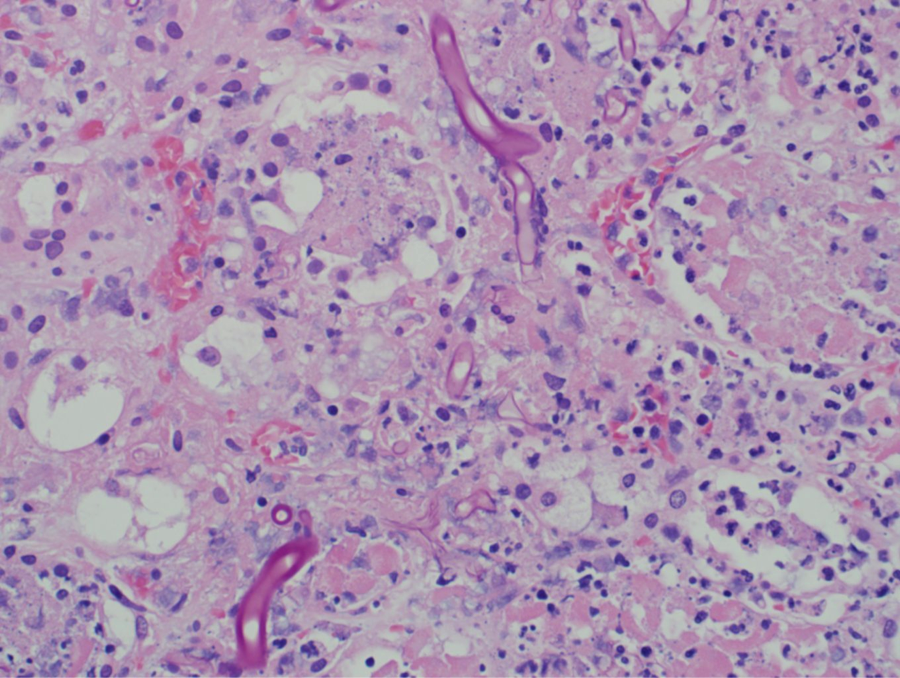
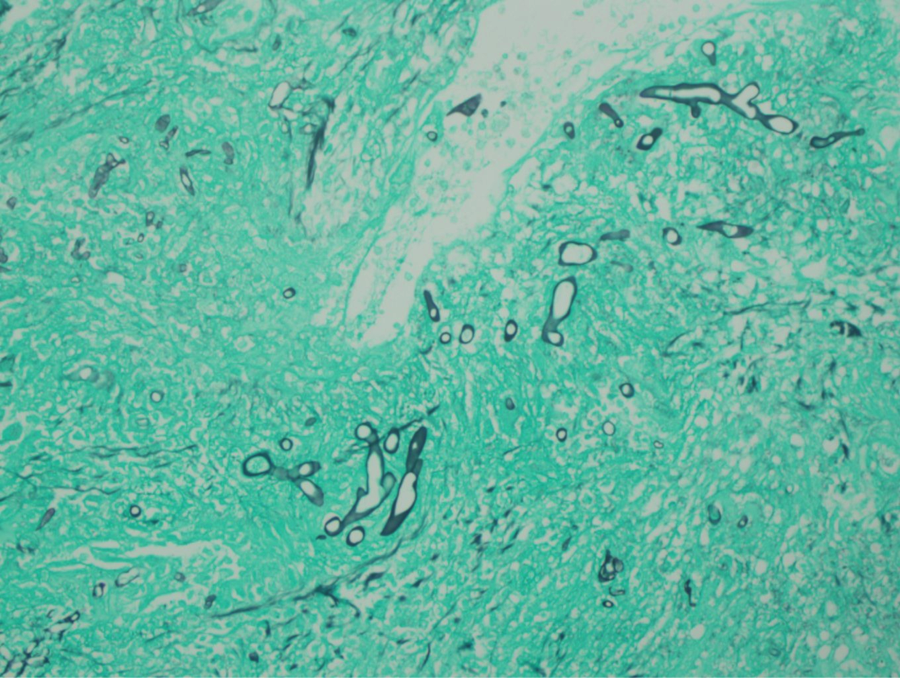
Case #13: H13-5186 Renal infarction post-kidney transplantation with fungal infection.
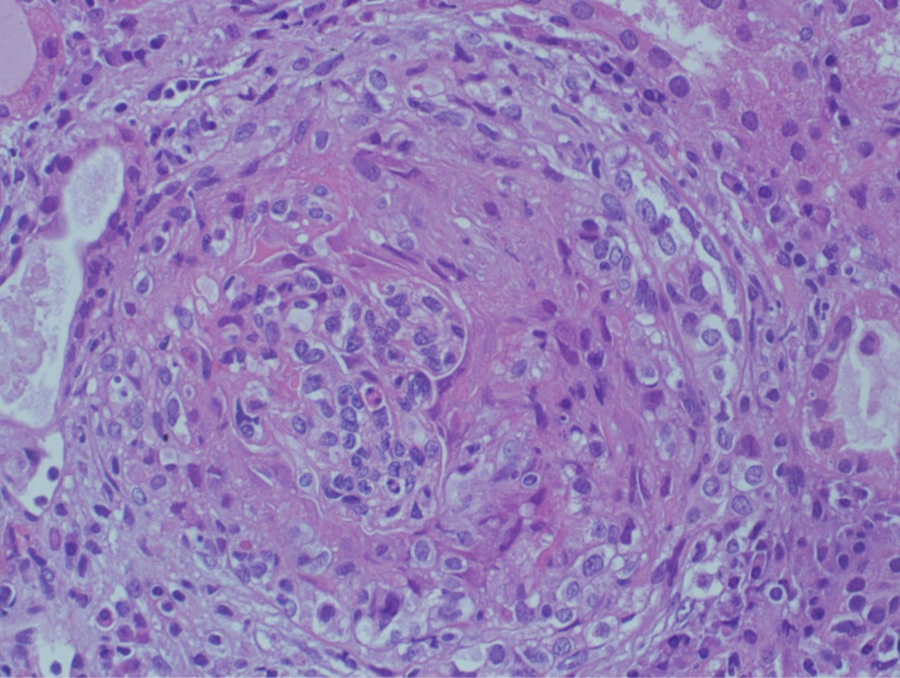
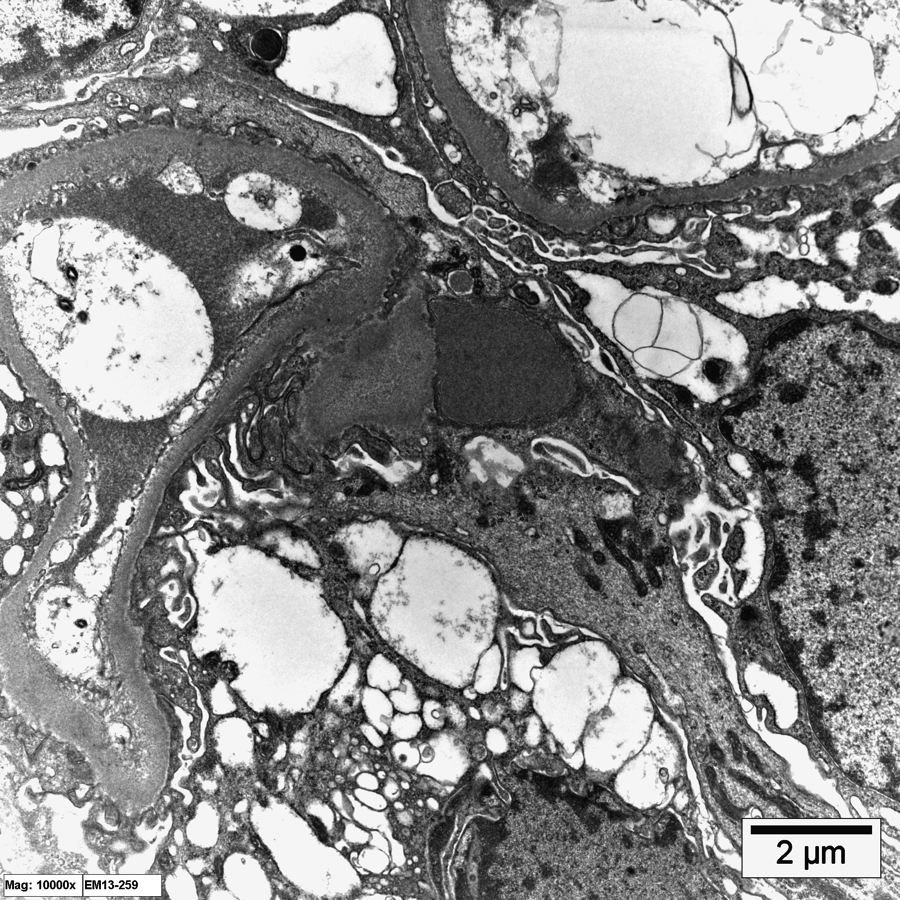
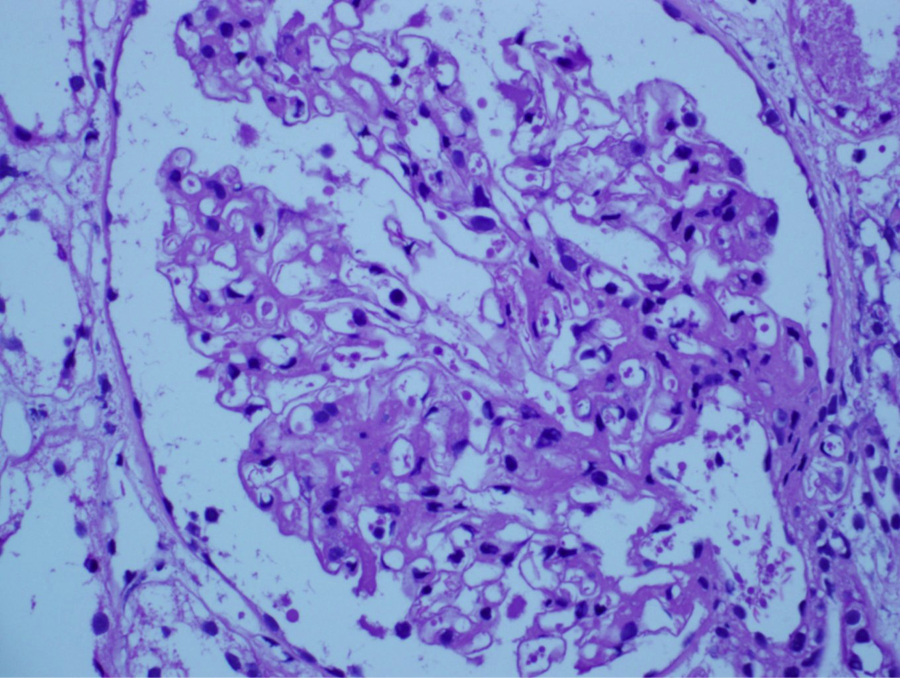
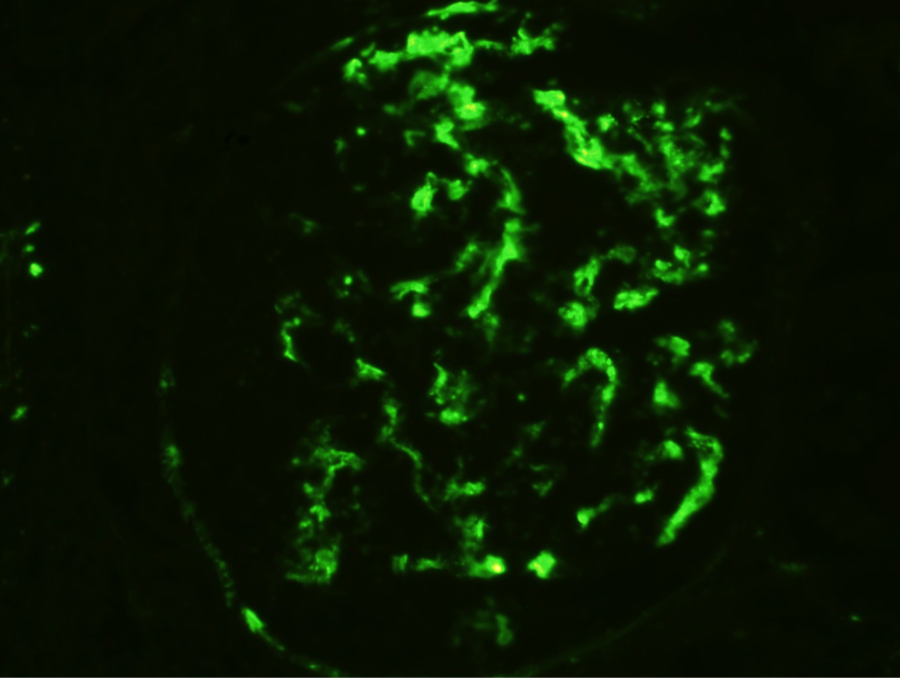
A 54 year old male presents with massive proteinuria and is found to have renal impairment(serum creatinine 2.5mg/dl). A renal biopsy is performed.
A 31 year old female who had kidney transplant 7 year ago for ESRD of unknown origin from LNRD presents with increased serum creatinine of 1.59mg/dl. A renal biopsy is performed.
A 46-year-old male patient with hypertension and diabetes mellitus is found to have proteinuria of 1.6g/24h. A renal biopsy is performed.
A 21-years-old female patient with small joint pain, fever, hair loss, proteinuria (2.1g/24h), hematuria, normal renal function, low C3. A renal biopsy is performed.
25-year-old female patient, a known case of SLE for 7 years, ANA positive, dsDNA positive, anticardiolipin (positive) 24h urine collection: with 1.6 g protein. A renal biopsy is performed.